1. 2 minutes of CPR (prime the pump)
2. Shock (120-200 J biphasic defibrillator)
3. RESUME CHEST COMPRESSIONS immediately following shock (to eliminate delays)
4. Check pulse (10 seconds during second round of chest compressions)
5. If no pulse: Shock 200 J
6. RESUME CHEST COMPRESSIONS immediately following shock
Tuesday, June 28, 2011
Friday, June 24, 2011
Local Anesthesia Toxicity (Lidocaine)
Local Anesthetic Agents Used Commonly for Infiltrative Injection

| Agent | Duration of Action | Maximum Dosage Guidelines (Total Cumulative Infiltrative Injection Dose per Procedure*) |
| Amides | ||
| Lidocaine (Xylocaine) | Medium (30-60 min) | Without epinephrine: 4.5 mg/kg; not to exceed 300 mg |
| Lidocaine with epinephrine | Long (120-360 min) | With epinephrine: 7 mg/kg |
| Bupivacaine (Marcaine) | Long (120-240 min) | Without epinephrine: 2.5 mg/kg; not to exceed 175 mg total dose |
| Bupivacaine with epinephrine | Long (180-420 min) | With epinephrine: Not to exceed 225 mg total dose |
| Bottom line Lidocaine 1% => 10mg per ml = Don't give more then 30 mls | ||
Thursday, June 23, 2011
Pediatic Resuscitation: SVT
Stable SVT
Vagal maneuvers:
Verapamil should not be used as blocking agent for in infants...Bradycardia and Hypotension

________________________________________
Unstable SVT:
Cardioversion:
Vagal maneuvers:
- Ice to face
- Blow through straw
- Initial: 0.1 mg/kg (max 6 mg)
- Susequant: 0.2 mg/kg (max 12 mg)
- Amiodarone: 5 mg/kg (over 20-60 min)
- Procainamide: 15 mg/kg (over 30-60 min)
Verapamil should not be used as blocking agent for in infants...Bradycardia and Hypotension

________________________________________
Unstable SVT:
Cardioversion:
- First dose: 0.5 - 1 J/kg
- Second dose: 2J/Kg
Monday, June 20, 2011






Sunday, June 19, 2011
Kawasaki's
My HEART
Mucosal involvement (strawberry tongue/fissured lips)
Hands (erythema palms/soles)
Eyes (conjuctivtis)
Adenopathy (cervical)
Rash: (usually trunk)
Temp: > 5 days
Criteria for Dx is Temp for 5 days and any 4 of the above
------------------------------------
Additional Mnemonic: CRASH and Burn
C-Conjunctivitis
R-Rash
A-Adenopathy
S-Strawberry tongue
H-Hand and feet swelling
Burn-fever for more than 5 days

Mucosal involvement (strawberry tongue/fissured lips)
Hands (erythema palms/soles)
Eyes (conjuctivtis)
Adenopathy (cervical)
Rash: (usually trunk)
Temp: > 5 days
Criteria for Dx is Temp for 5 days and any 4 of the above
------------------------------------
Additional Mnemonic: CRASH and Burn
C-Conjunctivitis
R-Rash
A-Adenopathy
S-Strawberry tongue
H-Hand and feet swelling
Burn-fever for more than 5 days

Saturday, June 18, 2011

Terrible T's: cyanoisis
Tetrology of Falot
a congenital heart defect which is classically understood to involve four anatomical abnormalities (although only three of them are always present). It is the most common cyanotic heart defect, and the most common cause of blue baby syndrome.
Tricuspid Atresia
Tricuspid fails to form (unopened). No blood flow from RA to RV. Tiny RV. Blood instead shunts across Foramen Ovale or ASD into Pulmonary Arterial system for oxygenation.

a congenital heart defect which is classically understood to involve four anatomical abnormalities (although only three of them are always present). It is the most common cyanotic heart defect, and the most common cause of blue baby syndrome.
Tricuspid Atresia
Tricuspid fails to form (unopened). No blood flow from RA to RV. Tiny RV. Blood instead shunts across Foramen Ovale or ASD into Pulmonary Arterial system for oxygenation.

Friday, June 17, 2011
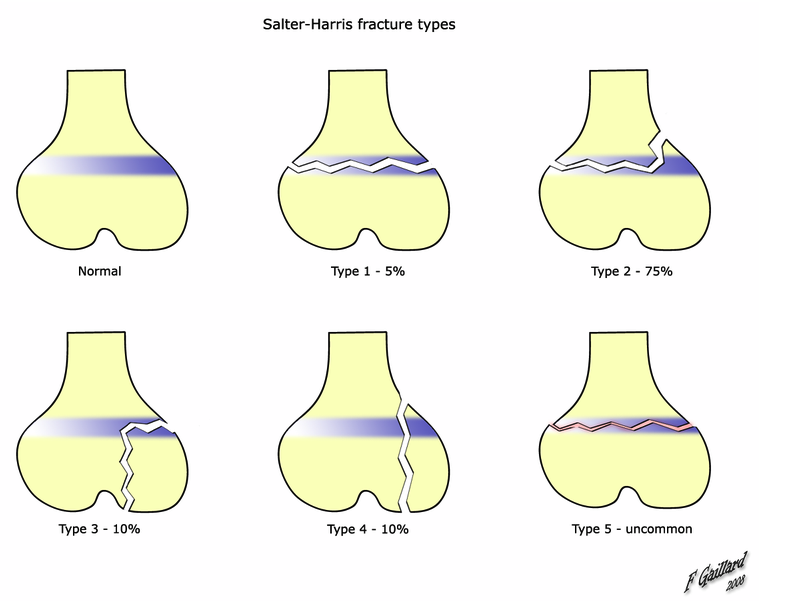
Salter Harris
SALTER mnemonic for classification
The mnemonic "SALTR" can be used to help remember the first five types. This mnemonic requires the reader to imagine the bones as long bones, with the epiphyses at the base.- I - S = Same (or Straight across). Fracture of the cartilage of the physis (growth plate)
- II - A = Above. The fracture lies above the physis, METAPHYSIS. (MOST FREQUENT 75%)
- III - L = Lower. The fracture is below the physis in the epiphysis.
- IV - T = Through. The fracture is through the metaphysis, physis, and epiphysis.
- V - R = Rammed (crushed). The physis has been crushed. (May dx on mechanism alone)
Thursday, June 16, 2011
Pediatric Fever
Historically, children aged 3 months to 3 years with rectal temperatures of 38.5o C (101.3 F) or higher had a risk of 2-4% for occult bacteremia.[1, 2] The leading cause of bloodstream infection was S pneumoniae, followed by H influenzae type b. With the introduction of effective vaccines for these pathogens, the incidence and epidemiology of childhood bacteremia in the immunologically normal host has changed.
The incidence of occult bacteremia in this population now ranges from 0.5-1%; moreover, 2 out of every 3 blood isolates from these children represent an artifact (contamination) and not a true pathogen.[3]S pneumoniae and E coli are the most common pathogens, accounting for two thirds of cases. In infants with S pneumoniae, many isolates are strains not covered by the currently available heptavalent conjugate vaccine.
Who do we need to get cath urine on???
Urine Cath Specimen: (from Boston Criteria for fever without focus)
< 6 month old males circumcised
<12 month old males uncircumcised
<24 month old females
The incidence of occult bacteremia in this population now ranges from 0.5-1%; moreover, 2 out of every 3 blood isolates from these children represent an artifact (contamination) and not a true pathogen.[3]S pneumoniae and E coli are the most common pathogens, accounting for two thirds of cases. In infants with S pneumoniae, many isolates are strains not covered by the currently available heptavalent conjugate vaccine.
Who do we need to get cath urine on???
Urine Cath Specimen: (from Boston Criteria for fever without focus)
< 6 month old males circumcised
<12 month old males uncircumcised
<24 month old females
Sunday, June 5, 2011


Saturday, June 4, 2011
Oxygen Dissociation Curve
http://en.wikipedia.org/wiki/Oxygen%E2%80%93haemoglobin_dissociation_curve
The causes of shift to right can be remembered using the mnemonic, "CADET, face Right!" for CO2, Acid, 2,3-DPG, Exercise and Temperature.[1] Factors that move the oxygen dissociation curve to the right are those physiological states where tissues need more oxygen. For example during exercise, muscles have a higher metabolic rate, and consequently need more oxygen, produce more carbon dioxide and lactic acid, and their temperature rises.
--------------------------------------------
CADET, face Right!
- CO2
- Acid
- 2,3-DPG(aka 2,3-BPG)
- Exercise
- Temperature

Friday, June 3, 2011
Asbestosis
Background
Pneumoconiosis is the general term for lung disease caused by inhalation and deposition of mineral dust.Pneumoconiosis caused by asbestos inhalation is called asbestosis. The word asbestos is derived from Greek and means inextinguishable, and asbestos is a group of naturally occurring, heat-resistant fibrous silicates. Asbestos fibers are long and thin (length-to-diameter ratio >3) and may be either curved or straight. The curved fibers are called serpentine (chrysotile is the prime example), and the straight fibers are amphiboles. Several different types of amphiboles (ie, amosite, anthophyllite, tremolite, actinolite, crocidolite) have been recognized. Chrysotile is by far the most common type of asbestos fiber produced in the world and accounts for virtually all asbestos used commercially in the United States.
Production and use of asbestos increased greatly between 1877 and 1967. In the 1930s and 1940s, scientists recognized a causal link between asbestos exposure and asbestosis. In the 1950s and 1960s, researchers established asbestos as a predisposing factor for bronchogenic carcinoma and malignant mesothelioma.
Note the image below.
 Asbestos pleural plaques.
Asbestos pleural plaques. Causes
In modern times, the risk to persons in the United States occurs mainly through the processing, manufacturing, and end-use of asbestos.
Manufacturers commonly use asbestos in the following products:
Manufacturers commonly use asbestos in the following products:
- Products containing asbestos cement - Pipes, shingles, clapboards, sheets
- Vinyl-asbestos floor tiles
- Asbestos paper in filtering and insulating products
- Material in brake linings and clutch facings
- Textile products - Yarn, felt, tape, cord, rope
- Spray products used for acoustical, thermal, and fireproofing purposes
- Insulation workers
- Boilermakers
- Pipefitters
- Plumbers
- Steamfitters
- Welders
- JanitorsImaging
Case 1. Postero-anterior (PA) chest radiograph in a 58-year-old man with a history of occupational exposure to asbestos shows right diaphragmatic pleural plaque calcifications, linear calcification along the left pericardium, and bilateral pleural plaques along upper ribs.
Case 4. The soft-tissue window setting of this chest computed tomography (CT) scan shows the envelope-like mass along the pleural surface surrounding the lung. This was a mesothelioma.
Pleural calcification
On chest radiographs, the prevalence of calcification in pleural plaques is reported to be 10-15%. In profile, calcified plaques appear as opaque lines that lie parallel to the chest wall, mediastinum, pericardium, and diaphragm. Viewed en face, calcified plaques are seen as irregular, heterogeneous densities, the so-called holly leaf. The presence of bilateral, superior diaphragmatic surface calcifications with clear costophrenic angles is virtually pathognomonic for asbestos-related pleural disease. (See the image below.)
A-a gradient
Alveolar-arterial gradient
| BMP/ELECTROLYTES: | |||
| Na+=140 | Cl−=100 | BUN=20 | / |
| Glu=150 | |||
| K+=4 | CO2=22 | PCr=1.0 | \ |
| ARTERIAL BLOOD GAS: | |||
| HCO3-=24 | paCO2=40 | paO2=95 | pH=7.40 |
| ALVEOLAR GAS: | |||
| pACO2=36 | pAO2=105 | A-a g=10 | |
| OTHER: | |||
| Ca=9.5 | Mg2+=2.0 | PO4=1 | |
| CK=55 | BE=−0.36 | AG=16 | |
| SERUM OSMOLARITY/RENAL: | |||
| PMO = 300 | PCO=295 | POG=5 | BUN:Cr=20 |
| URINALYSIS: | |||
| UNa+=80 | UCl−=100 | UAG=5 | FENa=0.95 |
| UK+=25 | USG=1.01 | UCr=60 | UO=800 |
| PROTEIN/GI/LIVER FUNCTION TESTS: | |||
| LDH=100 | TP=7.6 | AST=25 | TBIL=0.7 |
| ALP=71 | Alb=4.0 | ALT=40 | BC=0.5 |
| AST/ALT=0.6 | BU=0.2 | ||
| AF alb=3.0 | SAAG=1.0 | SOG=60 | |
| CSF: | |||
| CSF alb=30 | CSF glu=60 | CSF/S alb=7.5 | CSF/S glu=0.4 |
Equation
A-a gradient = PAO2 − PaO2[2]On Room air ( 21 % ) and at sea level, a simplified version of the equation is:
Aa Gradient = (150 - 1.2*(PCO2)) - PaO2
Values and meaning
The A-a gradient is useful in determining the source of hypoxemia. The measurement helps isolate the location of the problem as either intrapulmonary (within the lungs) or extrapulmonary (somewhere else in the body).A normal A-a gradient for a young adult non-smoker breathing air, is between 5-10 mmHg. Normally, the A-a gradient increases with age. For every decade a person has lived, their A-a gradient is expected to increase by 1 mmHg.
An abnormally increased A-a gradient suggests a defect in diffusion, V/Q (ventilation/perfusion ratio) mismatch, or right-to-left shunt.[3]
Because A-a gradient is approximated as: (150 - 5/4(PCO2)) - PaO2, the direct mathematical cause of a large value is that the blood has a low PO2, a low PCO2, or both. CO2 is very easily exchanged in the lungs and low PCO2 directly correlates with high minute ventilation; therefore a low arterial PCO2 indicates that extra respiratory effort being used to oxygenate the blood. A low PO2 indicates that at the patient's current minute ventilation (whether high or normal) is not enough to allow adequate oxygen diffusion into the blood. Therefore the A-a gradient essentially demonstrates a high respiratory effort (low arterial PCO2) relative to the achieved level of oxygenation (arterial PO2). A high A-a gradient could indicate a patient breathing hard to achieve normal oxygenation, a patient breathing normally and attaining low oxygenation, or a patient breathing hard and still failing to achieve normal oxygenation.
If lack of oxygenation is proportional to low respiratory effort, then the A-a gradient is not increased; a healthy person who hypoventillates would have hypoxia, but a normal A-a gradient
Subscribe to:
Comments (Atom)